
Reconstruction of the rotator cuff using a triple-row arthroscopic technique. Surgical technique
Reconstrucción del manguito rotador mediante técnica artroscópica de triple hilera. Técnica quirúrgica
Introduction
Rotator cuff repair seeks to restore shoulder function as quickly and painlessly as possible. Large, massive rotator cuff tears remain a major challenge for shoulder surgeons, to the extent that restoring the rotator cuff to its anatomical position can prove difficult(1). Failure rates of 10-30% have been reported in double-row or suture bridge arthroscopic repairs(2). Likewise, single-row fixation of massive rotator cuff tears has resulted in a re-rupture rate of up to 69% of the cases(3).
It is important to identify risk factors for further tears. In this regard, healing after surgery depends mainly on the quality of the tissue, the size of the tear, muscle atrophy and tendon retraction(4). Restoration of the footprint increases the likelihood of healing and subsequent physiological function of the shoulder(5). Maximising the contact area of the rotator cuff footprint improves the healing potential(6). We can predict the degree of involvement in the sagittal plane and retraction in the frontal plane based on the classification of Patte(7), muscle atrophy and fatty infiltration according to the criteria of Goutallier(8).
The most common approach to rotator cuff repair using an arthroscopic technique involves the use of suture anchors in a single-row configuration with anchors on the lateral aspect of the tendon footprint or a double-row strategy incorporating the same anchor configuration as the single-row repair, with the addition of a second row of anchors placed on the medial aspect of the tendon footprint(9).
Ostrander et al. proposed a modification of the double row or suture bridge technique in which an additional intermediate row is inserted independently of the medial and lateral rows (triple row). This variation of the technique was shown to result in a significantly greater native footprint contact surface and contact pressure compared to the double-row and equivalent transosseous techniques(6).
The present paper describes in detail the procedure of this increasingly popular technique that can be performed in a time not much longer than that of a standard suture bridge technique.
Surgical technique
Indications
The technique is indicated in large tears corresponding to sizes 1 and 3 of the Patte classification based on their extent(10), and retraction stages 2 and 3 in the frontal plane of the same classification(5,11). We do not use this technique for the repair of small tears, which can easily be repaired using simpler techniques. Likewise, we do not use this technique in cases that present: muscle atrophy and fatty infiltration (equal to or greater than Goutallier grade 3); subscapularis ruptures corresponding to grade II or higher in the Lafosse classification(8); patients subjected to previous operations; cases with signs of osteoarthritis; or patients with a lesser functional demand or who would not actively collaborate in the rehabilitation process.
Personally, we also tend to exclude patients with poor quality of the tendon (thinned, friable) or bone substrate (marked osteoporosis), where we opt for simpler techniques such as the single row procedure. We are often unable to assess these parameters until the very moment of joint and injury assessment, as indicated in Video 1.
reacae.31181.fs2310028en-video1.png
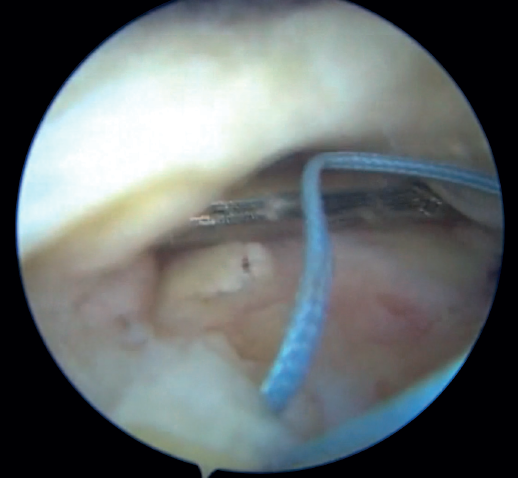
Video 1. Detailed step-by-step description of the triple-row technique for cuff reconstruction.
https://fondoscience.s3.eu-west-1.amazonaws.com/fs-reaca-videos/reaca.fs...
The magnetic resonance imaging (MRI) study prior to surgery allows us to assess the percentage of rupture according to the degrees of tendon retraction established in the Patte classification (Figure 1).
reacae.31181.fs2310028en-figure1.png
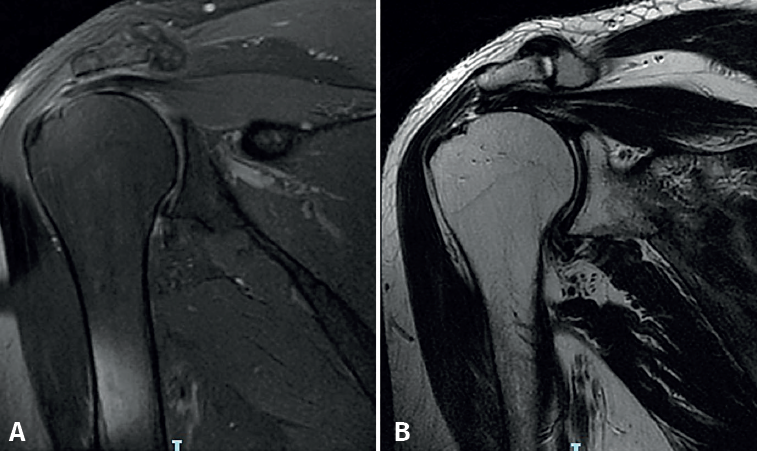
Figure 1. MRI study in the case (left shoulder) selected for this surgical technique. T1 (A) and T2 (B) sequences showing a Patte type 2 tear without significant muscle atrophy or fatty infiltration (Goutallier grade 0).
Surgical procedure
All patients undergo general anaesthesia and an ultrasound-guided regional interscalene nerve block by the Department of Anaesthesia.
The procedure is carried out analogously to other rotator cuff reconstruction techniques. The patient is placed in lateral decubitus with traction equivalent to 10% of the body weight. A pump with a mean pressure of 50 mmHg is used and controlled hypotension below 100 mm systolic blood pressure (SBP) is maintained to reduce bleeding and improve intraoperative arthroscopic vision.
Firstly, a classical posterior portal of the glenohumeral space is established, which allows us to assess the situation and determine the characteristics of the supraspinatus rupture and possible accompanying lesions of the subscapularis and the long portion of the biceps (LPB). The arthroscope is then reintroduced into the subacromial space through the same portal in the skin. The rest of the portals are under direct visualisation. The anterolateral, lateral and auxiliary anterosuperolateral (ASL) and posterosuperolateral (PSL) working portals are thus used.
Superficial debridement of the footprint over the greater tubercle of the humerus is then performed, the soft tissues are freed, and the tendon stump is mobilised with grasper-type forceps. This allows us to assess the size of the tear, the thickness of the tendon and the possibilities for reduction.
First step of the repair
In all cases, four perforations are made with the punch: two for the medial (or first) row and two for the central (or second) row. Next, the two bone implants of the central row are inserted, in this case Healicoil Regenesorb®4.5 with double suture using UltraBraid®N. 2 (Smith & Nephew Inc., Andover, MA, USA). Insertion is made close to the lateral margin of the footprint and at least 1 cm from the limit of the joint cartilage - one posterior and one anterior. These two implants constitute the second row that will allow reduction of the tear.
Additional anchors of the same type, i.e., Healicoil Regenesorb®5.5 with double suture using UltraBraid®N. 2 (Smith & Nephew Inc., Andover, MA, USA), are then placed at the margin of the joint cartilage. These anchors constitute the first row that will allow the tendon to be compressed over the footprint.
Second step of the repair
At the free margin of the tendon, four Loop Lasso®stitches are applied, according to the technique described by Lafosse(12). These stitches are made with each of the four strands of the two anchors of the second row, passing through the tissue using Curve®direct grasping forceps(Smith & Nephew Inc., Andover, MA, USA). Normally, the stitches are applied from posterior to anterior, always following the same order to avoid confusing them.
Then, the tendon is crossed 1 cm from its free margin with each of the 8 strands of the four sutures of the two anchors of the first row. The same Curve®direct grasping forceps are used for this purpose.
The lateral subdeltoid space is then debrided and the seat of the anchors of the third row is prepared.
Reduction phase in the second row (Figure 2A)
In the reduction phase in the second row, the tendon is reduced to its footprint by knotting the Loop Lasso®traction stitches at its free margin with the sutures of the anchors of the second or central row. The two strands of each suture are retrieved together in the subacromial space through the PSL portal for the posterior anchor and the ASL portal for the anterior anchor. Knotting is started at the most posterior suture while maintaining traction reduction of the anterior sutures. The type of knot used is the so-called easy knot, followed by half stitches to complete a "surgeon's knot" configuration. The same procedure is carried out successively on the other three sutures, and the remaining strands are cut.
reacae.31181.fs2310028en-figure2.png
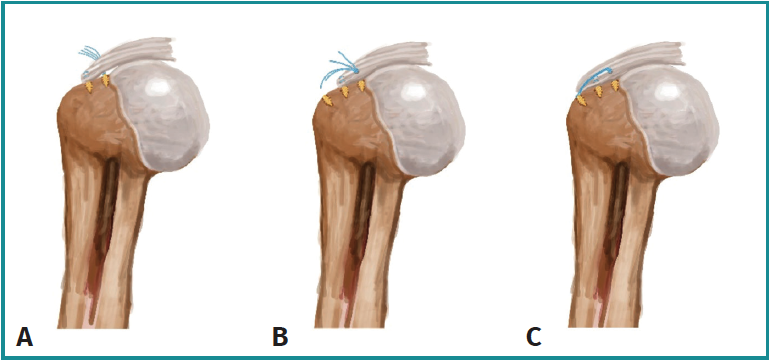
Figure 2. Illustration showing the effects achieved with each of the steps of the triple-row technique: A: reduction; B: compression of the footprint; C: tightening.
Compression phase in the second row (Figure 2B)
In this phase, the four sutures (8 strands) corresponding to the anchors of the first or medial row are knotted. For this purpose, the sutures of the posterior anchor will have been retrieved through the PSL portal and those of the anterior anchor through the ASL portal. The type of knot used at this stage is the slip knot (in our practice, the giant type), followed by three half safety knots. Only one of every two remaining strands is cut. In this way, an adaptation of the end of the tendon to the entire footprint will have been achieved.
Tightening phase in the third row (Figure 2C)
In this last phase involving tightening in the third row, the remaining four strands that have not been cut from the knots of the first row are recovered in criss-cross fashion. Each two of them are threaded into respective so-called "second-row" anchors without sutures. They are then slipped into the subacromial space with the aid of a metal hemi-cannula, and are inserted up to the mark in the previously made orifice. The sutures are tightened and clamped by threading the plunger on the anchors. The entire anchor is impacted, the insertion rod is removed, and the strands are cut. In this third row, we use FootPrint Ultra PK®(Smith & Nephew Inc., Andover, MA, USA) or Quattro® Link (Zimmer-Biomet, Zug) anchors. Finally, the result is assessed and the portals are sutured.
To date, no complications inherent to the surgical technique have been reported, and the difference in operating time has never exceeded 10 minutes compared to a double-row technique.
Postoperative period
A universal shoulder immobiliser is used for 3-4 weeks. During this period, pendulum-type and self-passive antepulsion exercises are allowed. Between weeks 4 and 8, passive exercises are indicated until full shoulder mobility is achieved. Once this has been achieved, between 6 and 12 weeks after surgery, depending on each case, progressive strengthening begins until an adequate balance is reached. Once this goal has been achieved, at around month 5 or 6, the return to sports or work activity(13)begins.
Advice and tips
We advise the described steps to be followed carefully, so that the technique as a whole is reproducible and practicable in a time not much longer than that of a standard suture bridge technique . Thus:
- Always follow a predetermined order in the insertion of the anchors, which should be the same for tissue transfixion and for knotting.
- Respect the indicated order of retrieval and knotting, so that each desired effect is obtained consecutively. Thus:
- Firstly, the mid-row anchors should anatomically reduce the rotator cuff tendon to the lateral margin of the native footprint using LoopLasso® or similar traction knots.
- Then, knotting of the anchors of the first or medial row must achieve the compression effect of the tendon to the footprint.
- Finally, the anchors in the third row must secure tightening of the entire reconstruction and increase the surface and contact pressure on the native footprint, thus reducing the stress required in the central row.
Discussion
The advantages of arthroscopic cuff repair over open repair include excellent visualisation of the tear anatomy, reduced morbidity and less postoperative pain(3,6).
The described technique secures a larger contact surface of the native rotator cuff footprint compared to the standard suture bridge and double-row techniques(1,3,6).
The ideal repair should be as anatomical as possible, with strong initial anchorage and reduced gap formation during the process of tendon integration into the bone. Biomechanical studies suggest the superiority of double-row (DR) techniques over single-row techniques in restoring the anatomical insertion footprint, as they increase the area of tendon attachment to the bone, thereby increasing the initial fixation strength(14).
Excessive pressure on the tendon can lead to devascularisation of local tissue and healing failure. Such high stress concentration may explain the increase in re-rupture rates, particularly medial to the anchors, as has been described over the last decade with the double-row or suture bridge technique(15).
A recent study by Park et al. has shown repair tension to be the most important factor for rotator cuff repair integrity. Consequently, the main objective is to suture the medial row on an anatomically reduced tendon without excessive tension. This is achieved by adding a repositioning anchor even before tying the medial row sutures (triple row concept)(13), thus reducing the re-rupture rate to 4.9%(1).
A study carried out by Trantalis et al. also showed 80% of new ruptures to be caused by failure of the medial row(16). This would explain that by reducing the tension on the medial row using a reduction anchor with this modified triple-row technique, the risk of repeat tearing due to suture constriction can be reduced(2). The integrity of a large, massive rotator cuff repair is closely related to the tension required to reach the joint margin of the footprint and the glenohumeral space with the reconstruction. Thus, it has been seen that the risk of a new rupture increases when a stress > 35 N(17) is required.
Several recent studies have compared different configurations and found that the described triple-row technique affords superior biomechanical performance, as well as a greater contact area and pressure distribution than the double-row or suture bridge technique(2,11,15). Mihata et al. reported a high failure rate in the treatment of large tears with both the single-row and the double-row techniques (62.5% and 41.7%, respectively). In the same study, the repeat rupture rate in the treatment of large tears using the triple-row technique was reduced to 7.5%(2).
The main advantage of the triple-row technique is tension-free knotting of the medial anchors, confirmed by mobilisation of the tendon with the forceps to the lateral margin of the native footprint. In contrast, in the single-row technique, the medial row anchors are knotted first, maximising the suture-tissue forces medially, which can lead to medial cuff failure(11). Thus, a double effect can be achieved with the triple-row technique: firstly, anatomical restoration of the footprint resembling double-row repair and, secondly, improved contact pressure and tendon compression similar to that seen with the suture bridging technique(15).
Conclusions
A detailed description is provided of this triple-row technique that can be performed in a time not much longer than that of a standard suture bridge or double-row technique.
Supplementary material
The video of the technique accompanying this article can be seen at (Video 1):
Figuras
Video 1. Detailed step-by-step description of the triple-row technique for cuff reconstruction.
https://fondoscience.s3.eu-west-1.amazonaws.com/fs-reaca-videos/reaca.fs...
Figure 1. MRI study in the case (left shoulder) selected for this surgical technique. T1 (A) and T2 (B) sequences showing a Patte type 2 tear without significant muscle atrophy or fatty infiltration (Goutallier grade 0).
Figure 2. Illustration showing the effects achieved with each of the steps of the triple-row technique: A: reduction; B: compression of the footprint; C: tightening.
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors Adrián Cuéllar Ayestarán and Ricardo Cuéllar Gutiérrez declare the following conflicts of interest: occasional collaboration contracts with Smith & Nephew.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- We are living a golden age in Spanish arthroscopic surgery
- Alteration of the coronal and sagittal axes of the knee and its implication in the failure of anterior cruciate ligament reconstruction. A systematic review
- Arthroscopic acetabular microfractures of the hip: survival and clinical outcome of the technique with a minimum follow-up of 5 years
- Hip arthroscopy provides medical personnel with an early and complete return to work. A multicentre study
- Novel articles on combined ligamentous injury of the anterior cruciate ligament and medial ligament complex of the knee
- Anteroinferior shoulder instability. Essential articles
- Treatment of shoulder instability with bone defects using a combination of arthroscopic bone block and <em>remplissage</em> techniques
- Reconstruction of the rotator cuff using a triple-row arthroscopic technique. Surgical technique
- Endoscopic treatment of calcific tendinitis of the gluteus maximus. A case report
- Incomplete discoid medial meniscus presenting coalescence with the anterior cruciate ligament
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.