
Single-row arthroscopic repair of isolated traumatic full-thickness subscapularis Lafosse IV tears
Reparación artroscópica en hilera simple de roturas traumáticas completas aisladas del subescapular Lafosse IV
Introduction
The subscapularis tendon is the largest and most powerful tendon of the rotator cuff and plays a key role in the shoulder as an internal rotator and anterior dynamic stabilizer of the joint. Superior rotator cuff injuries may be accompanied by low-grade subscapularis tears, however isolated subscapularis tears are infrequent and account for approximately 5% of rotator cuff tears(1,2). Isolated complete subscapularis ruptures are even more infrequent and usually occur after trauma in forced external rotation in abduction or forced extension of the arm. Surgical repair is generally indicated for acute, full-thickness, and repairable subscapularis tears, particularly in active patients, due to the tendon’s key role in strength and anterior stability. In chronic cases with significant retraction or fatty infiltration, surgery may still be considered to alleviate pain and improve residual function. Untreated complete tears can lead to persistent weakness in internal rotation, anterior shoulder pain, and progressive glenohumeral degeneration.
Historically, open repair was considered the gold standard for these injuries(3). However, arthroscopic advances in recent decades have favored the development of techniques and fixation methods for minimally invasive treatment of these tears. Nevertheless, arthroscopic treatment represents a technical challenge due to its location, tendon retraction and proximity to neurological structures(4). Due to its infrequency, the results of arthroscopic repair techniques for patients with complete traumatic ruptures of the subscapularis are poorly reported in the literature and are combined with results of open techniques or low-grade injuries. For high-grade lesions, although authors have recommended double-row fixation, clinical and biomechanical studies have found equivalence between this method and single-row repair(5,6).
Few studies have described the outcomes of Lafosse IV tears treated arthroscopically with a standardized single-row, two-anchor configuration, including the use of modern knotless fixation systems and high-strength suture tapes. The purpose of this study was to present the medium-term clinical outcomes of patients with isolated traumatic Lafosse IV subscapularis ruptures repaired arthroscopically in a single row. We hypothesized that this repair method would achieve satisfactory functional recovery with a low rate of complications.
Materials and methods
Informed consent was obtained for all patients included in this study and institutional review board approval form the institution was obtained (N0. 67. 03-03-24). A retrospective descriptive study was conducted of consecutive patients taken for arthroscopic rotator cuff repair by a single fellowship trained shoulder surgeon (M.L) between 2015 and 2022. Patients aged 18 to 80 years with isolated unilateral full-thickness subscapularis ruptures classified as Lafosse IV (complete rupture of the insertional tendon without subluxation and with ≤ Goutallier 3 fatty infiltration)(7) without posterosuperior rotator cuff involvement were included. Patients with follow-up of less than 24 months, glenohumeral osteoarthritis classified as Hamada > 3, anterior dislocation or subluxation, previous surgeries on the affected shoulder or neurological alterations were excluded.
Preoperative evaluation consisted of a standardized shoulder examination protocol conducted by the senior author (M.L.). Range of motion was assessed with a goniometer, including forward flexion, abduction, external rotation with the arm at the side, and internal rotation measured by the vertebral level reached with the thumb. Subscapularis integrity was tested with the modified belly-press test and the lift-off test, and findings were compared to the contralateral shoulder. Passive external rotation gain relative to the healthy side was documented, as increased values may indicate subscapularis insufficiency.
Radiological assessment included preoperative magnetic resonance imaging (MRI) of the affected shoulder, reviewed independently by the operating surgeon. MRI was used to confirm the diagnosis (Figure 1), classify the tear according to Lafosse classification, assess tendon retraction, fatty infiltration (Goutallier classification) on the sagittal plane, rule out advanced degenerative changes, and evaluate associated biceps pathology (Figure 1).
reacae.32385.fs2412027en-figure1.png
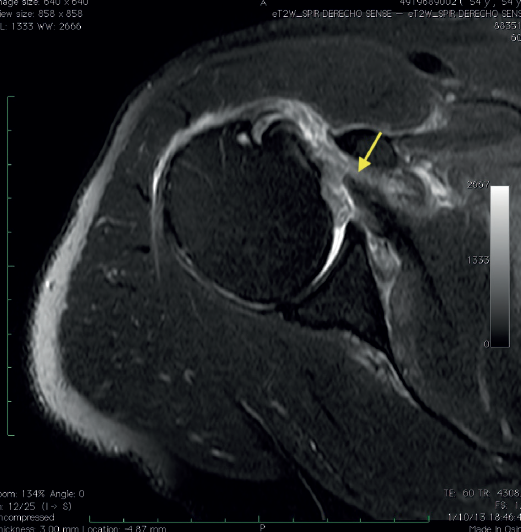
Figure 1. Axial magnetic resonance image of full-thickness acute subscapularis tear. Arrow: Torn subscapularis tendon.
Surgical indication was established for all patients presenting with acute or subacute isolated repairable full-thickness Lafosse IV subscapularis tears, in whom the tendon could be mobilized to the lesser tuberosity footprint without undue tension. Postoperative evaluation was performed at 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and annually thereafter. Demographic data, type of repair performed and complications were evaluated in all patients. The same standardized physical examination was used to evaluate range of motion, strength, and clinical signs of subscapularis integrity. Functional assessment was performed at final follow-up using the Single Assessment Numeric Evaluation (SANE) score(8). This scale is simple, quick to administer, and has shown good reliability in shoulder pathology, although it is less frequently used than other instruments such as the Constant or ASES scores.
At final postoperative follow-up, all patients underwent the same tests described in the physical examination to evaluate the integrity of the repair. Only in patients with clinical evidence suggestive of failure a control MRI was requested to assess the integrity of the repair.
Surgical technique
The same standardized repair technique was used in all patients by the same surgeon (M.L.) as explained herein below. Arthroscopic repair of the lesion is performed in the beach chair position under general anesthesia in combination with ultrasound-guided interscalene regional block. A pneumatic positioner is used to manage the limb. An initial arthroscopic exploration was performed. As working portals an anterior portal immediately lateral to the coracoid was developed through which an 8mm cannula is placed, as well as a viewing "outside the box" anterolateral portal(7) (Figure 2) and an accessory lateral portal for suture management (Figure 3). Using a 30° scope through the anterolateral portal, a bursectomy and debridement is performed using a curved blade shaver and radiofrequency around the lesser tuberosity and bicipital groove. The soft tissues are released with radiofrequency at the level of the rotator interval, on the anterior aspect of the tendon towards the anterior neck of the glenoid and in the posterolateral region of the coracoid until the tendon excursion is restored(4). In this step the axillary nerve and the superior and inferior subscapular nerves are identified during dissection in order to avoid inadvertent injury.
reacae.32385.fs2412027en-figure2.png
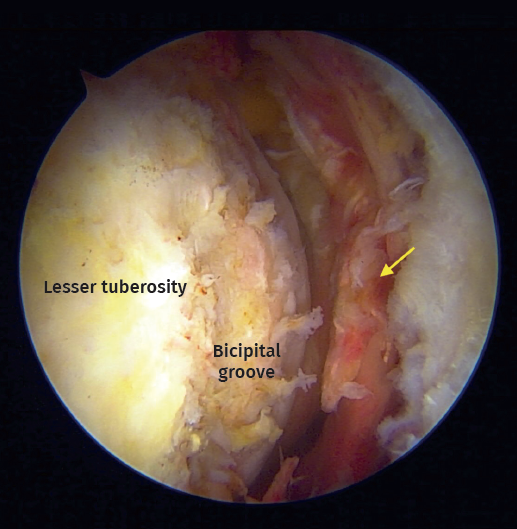
Figure 2. Arthroscopic view from anterolateral portal on a right shoulder in beach chair positioning. Chronic biceps tendon rupture. Arrow: Full-thickness and retraction of the subscapularis tendon
Next, the integrity and stability of the biceps is examined to determine whether to perform an intra-articular tenotomy or tenodesis using the inferior anchor of the repair and a double lasso technique (selected in patients under 60 years of age or with a slim build in whom the cosmetic result is relevant to prevent Popeye's deformity). Once the insertion footprint in the lesser tuberosity has been debrided, the lesion is repaired. In all cases a single row technique with two anchors (superior and inferior) is used. In some cases, both anchors were 5.5mm double loaded PEEK anchors (HEALICOIL PK 5.5mm, Smith and Nephew, Andover, MA) with a Mac stitch(9) using arthroscopic antegrade (bird's beak) forceps using an outside the box visualization technique. In the most recent cases, a hybrid fixation technique was employed, securing two arthroscopic tapes (ULTRATAPE, Smith and Nephew, Andover, MA) positioned in luggage tag configuration, anchoring them to a 5.0 mm PEEK knotless anchor (HEALICOIL knotless PK, Smith and Nephew, Andover, MA) on the inferior portion of the lesser tuberosity footprint (Figure 4).
reacae.32385.fs2412027en-figure3.png
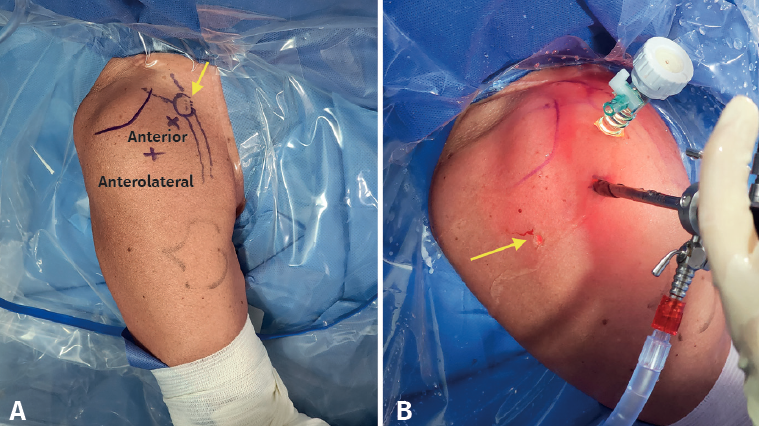
Figure 3. Intra-operative (A) marking of arthroscopic portals for arthroscopic repair of subscapularis injuries (B) Arthroscopic lens through anterolateral portal, 8mm cannula at the anterior portal. Arrow: accessory portal to manage sutures.
All patients followed the same rehabilitation protocol. After the procedure, immobilization in a sling is performed for 5 weeks, initiating passive mobility on week 3, avoiding external rotation in the initial phase until week 5. At the 6th week active mobility is authorized and after 8 weeks when mobility is complete, strengthening exercises are commenced. Between 6 and 12 months after the procedure, patients have returned to daily and work activities.
reacae.32385.fs2412027en-figure4.png
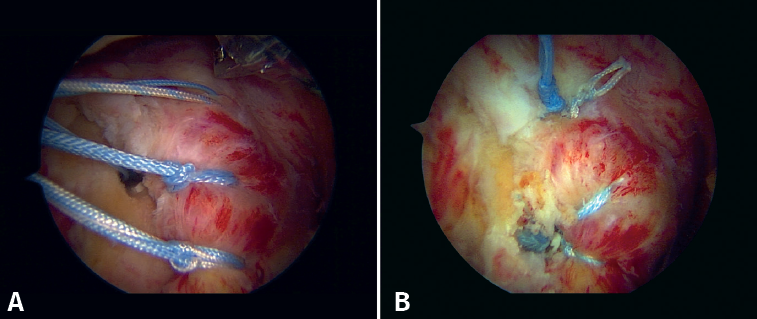
Figure 4. Arthroscopic “outside the box” view of single-row subscapularis hybrid repair using a knotted anchor superiorly with a Mac stitch and a knotless anchor inferiorly with luggage tag suture tapes. a) Before knot tying and tape fixation. B) Final repair with knotless inferior anchor.
Statistical analysis
Data was entered into a database created in Microsoft Excel for later analysis in JASP statistical analysis software. The data are described using absolute and relative frequencies for qualitative variables, and means, ranges and standard deviations for quantitative variables.
Results
During the period described, a total of 15 patients who met the inclusion criteria were intervened. One patient was excluded due to insufficient follow-up time. A total of 14 patients were included (Table 1), with an average age of 65 years (range 46 to 76 years), 8 of whom were men (57%). The average follow-up time was 29.4 months (range 24 to 41months). Of the 14 patients who were evaluated, 13 (92.8%) had some compromise of the proximal biceps such as partial ruptures, degenerative lesions or medial instability (Figure 5). Biceps tenotomy was performed in 9 patients (64.2%), an intra-articular tenodesis in two cases (14.2%), and a chronic biceps rupture was found in two (14.2%) patients. In half of the patients (7) the subscapularis tear was repaired with two knotted anchors, and in the remaining with a hybrid fixation using a knotted superior anchor and a knotless inferior anchor with suture tapes (Table 2).
reacae.32385.fs2412027en-table1.png
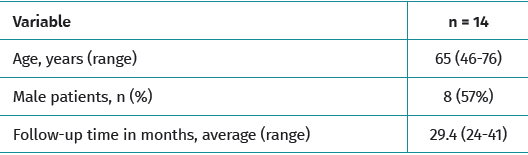
Table 1. Baseline patient demographics
At final follow-up, 10 patients (71.4%) achieved complete functional and mobility recovery, with negative belly-press and lift-off tests and no anterior shoulder pain. The mean SANE score was 80.3% (±22.3).
reacae.32385.fs2412027en-figure5.png
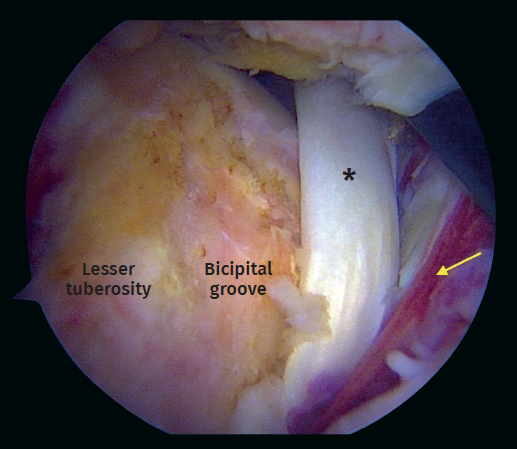
Figure 5. Arthroscopic view. Full-thickness subscapularis tear with medial instability of the long head of the biceps tendon. Asterisk: biceps tendon. Arrow: torn subscapularis tendon.
Three patients (21.4%) sustained a re-rupture of the subscapularis tendon after new traumatic episodes occurring more than 6 months postoperatively. All three had positive lift-off and belly-press tests, an external rotation increase of at least 15° compared to the contralateral side, and MRI confirmation of tendon failure. One of these patients was managed conservatively with physical therapy and corticosteroid injection, while the remaining two underwent revision to reverse total shoulder arthroplasty. Of the three re-ruptures, two occurred in repairs with knotted anchors and one in a hybrid fixation.
reacae.32385.fs2412027en-table2.png
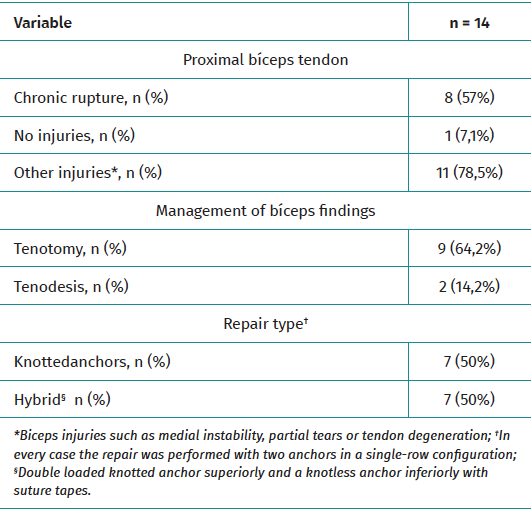
Table 2. Arthroscopic findings and type of repair
No patient experienced postoperative infection, neurovascular injury, anchor loosening, or adhesive capsulitis. One patient (7.1%) reported persistent anterior shoulder pain without loss of function, which was successfully managed with a single subacromial corticosteroid injection
Discussion
The main finding of this study is that arthroscopic repair with two anchors in a single-row configuration for high-grade full-thickness subscapularis tears yields satisfactory clinical outcomes at medium term follow up. Clinical complications with recurrence of symptoms in this case series occurred after new traumatic episodes and were not associated with the type of fixation (knotted or knotless) used for repair.
Although open repair was the gold standard for repairing subscapularis injuries, advances in arthroscopic techniques and instrumentation have made it possible to offer favorable minimally invasive results in these patients, offering superior results in range of motion and function(10).
Although different authors have usually recommended double-row fixation for high-grade full-thickness subscapularis tears, recent studies have found no difference in results when comparing both types of fixation. Our outcomes align with those reported by Yoon et al., who found no significant difference in clinical results or re-tear rates between single- and double-row repairs of isolated subscapularis tears at two-year follow-up(11). When analyzing the biomechanical characteristics of both techniques, there is still insufficient evidence to prove the superiority of single or double row fixation for repairing subscapularis tears(12). Similarly, Xiao et al. in a systematic review of 811 studies found that 89% of subscapularis repairs are fixed in a single-row configuration, and there is no difference in terms of clinical outcome or integrity of repair between single and double-row repair(13). Therefore, we decided to repair full-thickness subscapularis tears in a single-row given the equivalence in clinical and biomechanical outcomes in contrast with the disadvantages of a double-row fixation in terms of cost, surgical time and technical difficulty.
The use of arthroscopic suture tapes has demonstrated superior biomechanical properties when compared to traditional round sutures, providing greater load to failure and less tendon displacement with applied loads(6). For this reason, the authors have chosen theses type of fixation in the most recent cases using hybrid fixation with knotted anchors in the superior region of the tendon and knotless fixation with tapes inferiorly. Knotless fixation may also reduce the risk of knot impingement and facilitate more uniform tensioning of the repair. In our cohort, re-ruptures occurred in both knotted and hybrid constructs, suggesting that patient-related and trauma-related factors played a more significant role in repair failure than the fixation method itself.
Given the technical demands of subscapularis repair and the rarity of isolated Lafosse IV lesions, surgical strategy should balance biomechanical robustness with procedural efficiency. Our findings suggest that a single-row, two-anchor repair—especially when augmented with modern knotless technology and suture tapes—can achieve favorable functional outcomes while minimizing complexity.
This study has several limitations, as it is a retrospective case series design with no comparator group. A small sample size is the main limitation of this study, nonetheless we decided to use strict inclusion criteria given the infrequency of presentation of isolated high-grade traumatic subscapularis ruptures. No randomization of surgical techniques was performed and the results of two types of repair (knotted anchors exclusively and combined with knotless anchors) are presented due to the modification of the surgical technique decided by the surgeon over time. We did not use routine control MRI in our practice, so we did not evaluate the outcome of tendon healing in images. Also, clinical tests to assess tendon integrity are subjective for both patient and examiner. Future studies may compare these two techniques in randomized research designs to evaluate their benefits.
Conclusions
In a medium-term follow-up, arthroscopic repair with two anchors in a single-row of isolated full-thickness traumatic injuries of the subscapularis achieved satisfactory clinical outcomes. Symptomatic re-ruptures in this group of patients were caused after new traumatic episodes.
Figuras
Figure 1. Axial magnetic resonance image of full-thickness acute subscapularis tear. Arrow: Torn subscapularis tendon.
Figure 2. Arthroscopic view from anterolateral portal on a right shoulder in beach chair positioning. Chronic biceps tendon rupture. Arrow: Full-thickness and retraction of the subscapularis tendon
Figure 3. Intra-operative (A) marking of arthroscopic portals for arthroscopic repair of subscapularis injuries (B) Arthroscopic lens through anterolateral portal, 8mm cannula at the anterior portal. Arrow: accessory portal to manage sutures.
Figure 4. Arthroscopic “outside the box” view of single-row subscapularis hybrid repair using a knotted anchor superiorly with a Mac stitch and a knotless anchor inferiorly with luggage tag suture tapes. a) Before knot tying and tape fixation. B) Final repair with knotless inferior anchor.
Figure 5. Arthroscopic view. Full-thickness subscapularis tear with medial instability of the long head of the biceps tendon. Asterisk: biceps tendon. Arrow: torn subscapularis tendon.
Tablas
Table 1. Baseline patient demographics
Table 2. Arthroscopic findings and type of repair
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The author Dr. Mauricio Largacha declare the following conflicts of interest: Consultant Smith and Nephew.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- Aprender artroscopia
- Resultados funcionales y clínicos del tratamiento artroscópico de la epicondilitis lateral
- Resultados similares entre la reparación y no reparación de la capsulotomía interportal a 3 años de seguimiento mínimo tras artroscopia de cadera como tratamiento del choque femoroacetabular. Estudio del Grupo Ibérico de Preservación de Cadera
- Balón subacromial y tenotomía de la porción larga del bíceps vs. tenotomía aislada en pacientes con rotura masiva irreparable de manguito rotador. Resultados funcionales a medio plazo
- Reparación artroscópica en hilera simple de roturas traumáticas completas aisladas del subescapular Lafosse IV
- Single-row arthroscopic repair of isolated traumatic full-thickness subscapularis Lafosse IV tears
- Ligamentoplastia y <em>remplissage</em> en la luxación anterior recidivante de hombro: protocolo, técnica y resultados en nuestro centro
- Desgarro parcial del peroneo corto como complicación tras la cirugía de inestabilidad lateral del tobillo: informe de caso
- Resección artroscópica de quiste sinovial del ligamento cruzado anterior: a propósito de dos casos
- In memoriam Dr. Ricardo Cuéllar Gutiérrez
- Los cruzados anteriores: hermanos de sangre
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.